Ongoing projects
Epidemic elimination dynamics
I'm currently wrapping up a project on epidemic elimination and reemergence dynamics induced by vaccine hesitancy/fatigue or enforce-and-relax vaccination policies, in collaboration with R Breban (Institut Pasteur, France) and R Vardavas (United States). I developed a stochastic model of smallpox transmission to estimate the times to eradication (C++, Python). We apply and discuss our results in the context of measles outbreaks and elimination efforts.
Modeling tuberculosis epidemiology
This is a self-directed study of tuberculosis epidemiology and infectious disease modeling, built as both a learning record and a portfolio piece. It combines an overview of TB natural history, burden, and modeling approaches with a Python SELT(R)-style toy model, currently under development. The full repository, including notes on using AI-assisted workflows for the work and a set of Cursor plans to reproduce a similar project for another disease, live at github.com/sjijon/learning-tb-modeling.
This project inspired the creation of a template repository for building a structured workflow to learn about the epidemiology, ongoing global programs and modeling approaches (including the development of a toy model) of an infectious disease, especially when they have little or no prior experience with that disease. The template is available at github.com/sjijon/ai-plans-for-learning-infectious-disease-modeling-repo.
Past projects (selected)
Estimating the date of emergence of epidemic outbreaks, using early case data
Paper (PLOS Comp Bio, 2024) |
Code (Julia for simulations, R for figures)
We developped a stochastic branching-process model to estimate the date of emergence of epidemic outbreaks, using available case data. We calibrated using data on the first reported sequences of the Alpha variant and then applied the model to different datasets of early COVID-19 reported cases. We compared our estimates with the dates of emergence reported in the literature.
Our main results show that the date of emergence of an epidemic outbreak can be estimated using early detection data, even when the data is incomplete. We found that our estimates are consistent with the dates of emergence reported in the literature, and that our model is computationally efficient compared to other approaches such as Approximate Bayesian Computation (ABC).
Fig. Estimated date of emergence of COVID-19.
Our model results compared with results from the literature, as well as the results from an ABC model.
SARS-CoV-2 infection risk among healthcare workers in quarantine-hospitals
Paper (Sci Rep, 2022) |
Code (R)
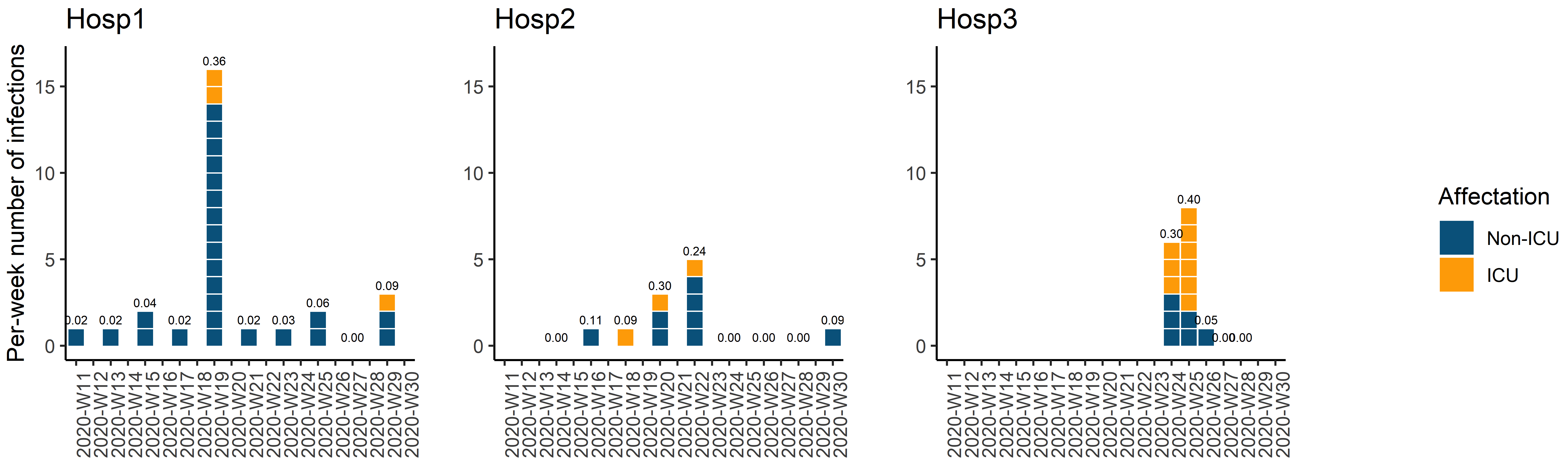
The aim of this project was to estimate the SARS-CoV-2 infection risk among healthcare workers (HCWs) participating in the quarantine-hospital intervention established by the Egyptian government during the first wave ofthe COVID-19 epidemic. Our model is calibrated using detection data of 3 hospitals, accounts for RT-PCR false negatives and unveils the share of undiagnosed infections.
The model-based incidence rates yielded the per-shift infection probabilities of ~13.7% and 23.8% for Hosp1 and Hosp2, respectively, and ~42.6% for Hosp3. We estimated 45–59% of infections were undiagnosed. Risk tended to be higher in non-ICU units in two hospitals but higher in ICU in the third hospital, which operated as a quarantine hospital for shorter time and shorter shifts than the other two hospitals.
Fig. Case data of three Egyptian COVID-19 quarantine-hospitals.
HCWs worked 2-week shifts in two hospitals and 1-week shifts in the third.
HIV elimination under voluntary PrEP adoption
Paper (AIDS, 2021) |
Code (Matlab)
My PhD research project focused on infectious diseases models accounting for voluntary adoption of preventive methods, using a game-theoretical approach. One of the applications we explored was pre-exposure prophylaxis uptake to prevent HIV infection among men who have sex with men at high risk of HIV infection. This project contributed to the analyses of the impact on PrEP in target populations at early estages of PrEP rollout in Paris (2015), and was developeed in the context the WHO elimination goals for 2030.
Our model was calibrated to reproduce HIV epidemic numbers for the population of MSM in Paris. The simulations return PrEP uptake resulting from the utility maximisation of individuals. We found that PrEP uptake can be caracterised by a three-region behavior: when PrEP is perceived as too costly, individuals do not use PrEP (region III); with decreasing perceived cost, uptake increases (region II) and HIV elimination in the long term can be reached if PrEP coverage is above a certain threshold (region III, stripes), which requires individuals to perceive PrEP cost to be low, even under very high levels of effectiveness. However, we found that there is no equilibrium in region III, which means that the system is unstable and continous efforts to maintain cost perceived as low are required to reach and maintain elimination status.
Fig. PrEP coverage resulting from utility maximisation.
Here, PrEP coverage is depicted as a function of PrEP effectiveness and the cost perceived for PrEP relative to the cost of being treated for HIV in case of infection.
Updated: January, 2026.